Andrew Sullivan nicely lays out the health care dilemma:
In 2011 we live in a world even our parents could barely dream of. We have the medical capacity to bring Gabby Giffords back to life even after a bullet has gone straight through her brain; we have the scientific ability to model a retrovirus on computers and get to real world treatments in years rather than decades; we are able to give wounded soldiers new limbs and tell cancer patients that hope is real and not be lying. We can map the human genome and devise revolutionary new treatments for previously fatal conditions; and we can extend life beyond any previous human generation's imagination.
...At the same time, as a matter of economics and mathematics, we also know at the back of our minds that we simply cannot give it to all - because these breakthroughs involve huge investment, highly trained experts, and inherently expensive technology. And as the options for health grow, we are forced to make choices that were previously out of our grasp, and those choices make us, in some way, gods. We collectively decide who can live for how long and who can die - because for the first time in human history we really have that choice. In fact, we have no escape from that choice.
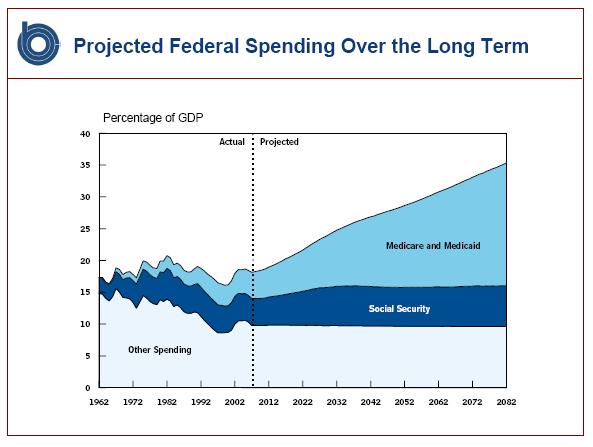
Indeed, we must choose because continuing down the current path will bankrupt the federal government. President Obama describes the situation in less abstract terms:
When my grandmother got very ill during the campaign, she got cancer; it was determined to be terminal. And about two or three weeks after her diagnosis she fell, broke her hip. It was determined that she might have had a mild stroke, which is what had precipitated the fall.
So now she’s in the hospital, and the doctor says, Look, you’ve got about — maybe you have three months, maybe you have six months, maybe you have nine months to live. Because of the weakness of your heart, if you have an operation on your hip there are certain risks that — you know, your heart can’t take it. On the other hand, if you just sit there with your hip like this, you’re just going to waste away and your quality of life will be terrible.
And she elected to get the hip replacement and was fine for about two weeks after the hip replacement, and then suddenly just — you know, things fell apart.
I don’t know how much that hip replacement cost. I would have paid out of pocket for that hip replacement just because she’s my grandmother. Whether, sort of in the aggregate, society making those decisions to give my grandmother, or everybody else’s aging grandparents or parents, a hip replacement when they’re terminally ill is a sustainable model, is a very difficult question. If somebody told me that my grandmother couldn’t have a hip replacement and she had to lie there in misery in the waning days of her life — that would be pretty upsetting.
THE NEW YORK TIMES: And it’s going to be hard for people who don’t have the option of paying for it.
THE PRESIDENT: So that’s where I think you just get into some very difficult moral issues. But that’s also a huge driver of cost, right?
I mean, the chronically ill and those toward the end of their lives are accounting for potentially 80 percent of the total health care bill out here.
THE NEW YORK TIMES: So how do you — how do we deal with it?
THE PRESIDENT: Well, I think that there is going to have to be a conversation that is guided by doctors, scientists, ethicists. And then there is going to have to be a very difficult democratic conversation that takes place. It is very difficult to imagine the country making those decisions just through the normal political channels. And that’s part of why you have to have some independent group that can give you guidance. It’s not determinative, but I think has to be able to give you some guidance. And that’s part of what I suspect you’ll see emerging out of the various health care conversations that are taking place on the Hill right now.
This pretty well sums matters up, and towards the end the president outlines his preferred solution: the establishment of a learned panel of wise men and women, appointed by the government and empowered to determine which people to deserve access to health care. Since this 2009 interview was given the idea of such a committee has moved from abstraction into reality, and is now known as the Independent Payment Advisory Board.
Greg Mankiw contrasts this approach with that offered by Rep. Paul Ryan:
Ryan proposes that seniors use their "premium support"[i.e. subsidies] to shop among competing private insurers. Here we see the fundamental differences between the parties: One believes in spending more and allocating that spending via central planning. The other believes in spending less and harnessing individual choice and competition to ensure that the money is spent wisely.
Beyond the insurance subsidies proposal offered by Ryan, other possibilities have been floated that are in a similar vein, such as offering cash grants to seniors.
In arguing for the central planning in his deficit speech this week, the president deplored Ryan's proposal, vowing he would not "leave seniors at the mercy of the health insurance industry." Left unsaid is that Obama's preferred policy would leave seniors at the mercy of bureaucrats and waning capabilities of the US Treasury. There is no system in which everyone gets all of the health care that they want.
Supporters of the president's approach will likely counter that while this may be accurate, their system would be more moral or just, as access to health care would not depend on something so gauche as money. But is this so? Using Obama's example of his grandmother, let us say that a government committee decided that taxpayer money should not be spent on elderly cancer-stricken grandmothers in need of hip replacements. How is that morally preferable to a situation in which the same grandmother simply ran out of money and could not afford the procedure? Do not tell me that it is permissible because we as society decided collectively. "We" most certainly did not -- a group of government appointees did.
Let us imagine, however, that the powers that be decided Obama's grandmother, who otherwise couldn't afford a hip replacement, would be granted one at taxpayer expense -- government at its most compassionate, no? But it is still not apparent that this is morally correct. Why does the grandmother enjoy a claim on the resources of others for her health care needs? Why should thousands of dollars be taken from others so that grandma can have her life extended or improved for another few weeks, months or even years simply because of a committee's decision? The people this money was taken from may have had big plans for it. Why should their consumption be reduced in order to extend the lives of others?
I suspect that the response offered by many people would go something along the lines of "Because human life is priceless and we can't simply let people die." But this is nonsense. Life does have a price on it and death is inevitable -- at best it can only be delayed.
It's no secret that everyone, should they be fortunate enough, will grow old, become more susceptible to health problems, and will ultimately expire. Every dollar we consume now is one less dollar available to treat those health problems later on. How we spend those dollars, now or later, is a choice we all make. Maybe we decide that it is best to enjoy money in the present, and take a trip to Hawaii instead of a knee replacement when we are 80. That's a valid choice. But we also can't have a system where we spend the money now, grow old, and then expect the right to consume all the health care we want and have it paid for by others.
While I am not convinced that Paul Ryan has arrived at the best possible solution for the problems that plague Medicare, he at least moves the needle in the right direction. We simply must implement reforms that limit the government's exposure and provides an incentive for patients to be judicious about their health care consumption. Ryan's plan holds at least the possibility of accomplishing this in some fashion. The president's does not.

{kind=link}
No comments:
Post a Comment